The current paradigm of perception of the musculoskeletal apparatus and its regulation entails a deeply ingrained opinion on the possibility of “programming the basic motor functions”. I think a program of such complexity, which would resemble the one that regulates the human locomotion, has not yet been created artificially. Rather than create a new one, we are more able to talk about the possibility of repairing the existing program. It’s not about creating a substitute program – there is always a genetically coded and “intrinsically given” program that would be used. It could be its developmentally older program part or the developmentally younger program part.
Eventually, there is a possibility of running the genetically given program that has been inactive and dormant. It is necessary to distinguish between the programs that are responsible for the basic regulation of the musculoskeletal apparatus and the programs that enable motor learning
Motor abilities have to be perceived as a form of function of the central nervous system. The regulation of the human musculoskeletal apparatus based on the clinical experience with the Vojta method seems to be close to the regulation of systems that are intrinsically complex, vast, morphologically soft, weakly constructed or otherwise unspecified. Similarly to the musculoskeletal apparatus of the humans, these systems are composed of many various parts with several mutual confused relations. They interact mutually by complex and scarcely comprehensible algorithms.
Neuronal Regulation of the Musculoskeletal Apparatus – Its “Software”
For better comprehension, I will try to illustrate the view of the program regulating the human motor skills by using a metaphor that would compare the programs of the human body to the programs that control a computer.
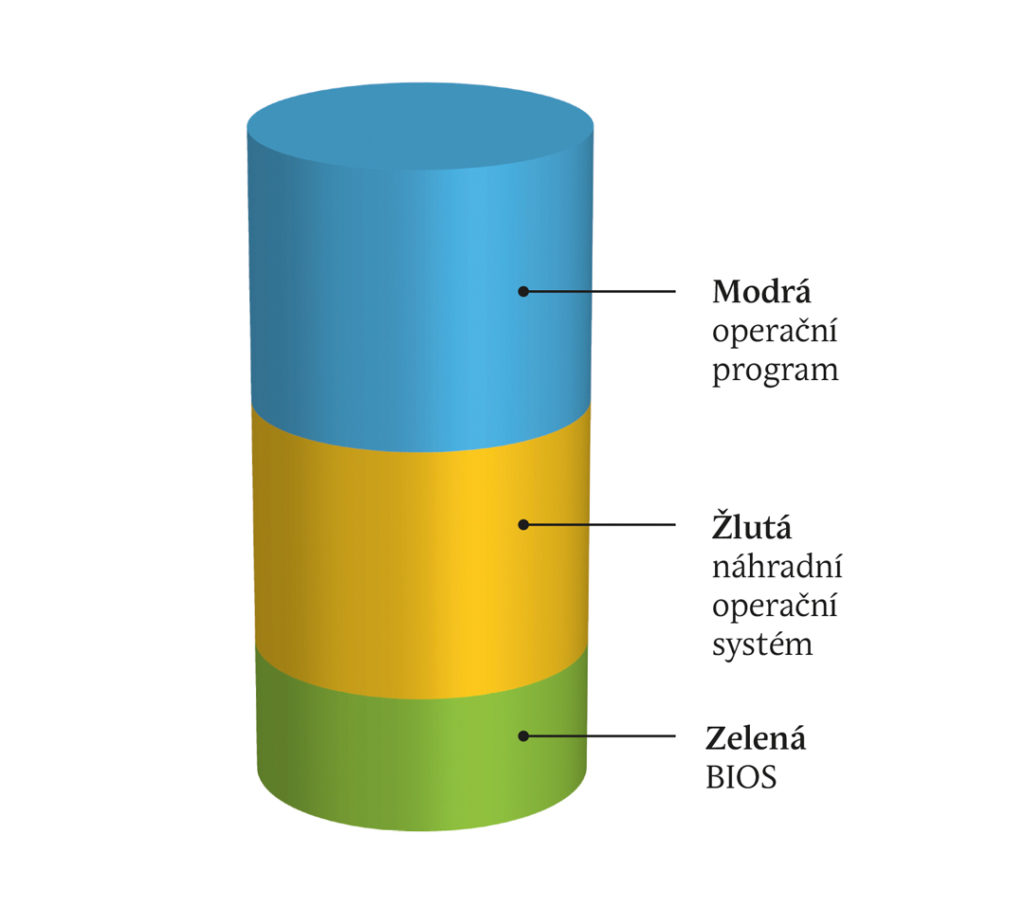
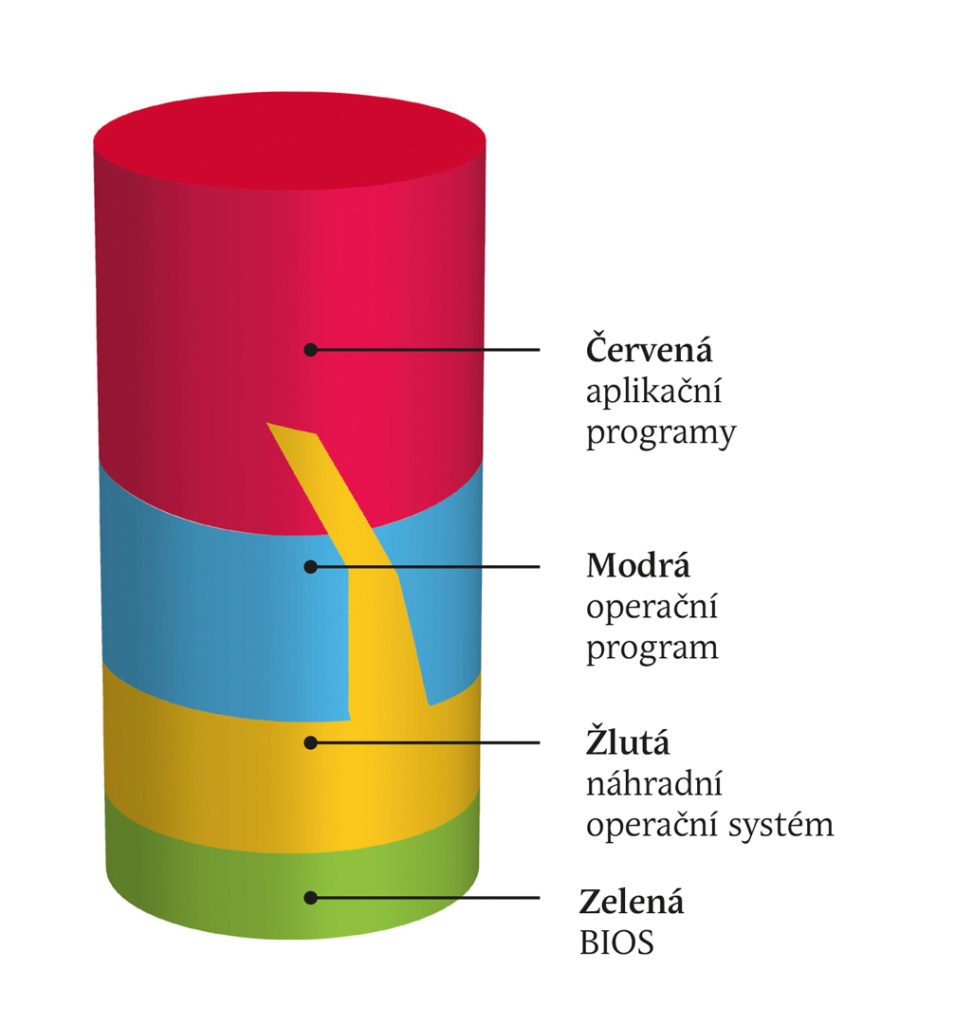
BIOS
Like a computer, the human brain has a quite elementary start up BIOS program, which an ordinary computer user does not come in contact with it.
BIOS is a system providing the most elementary functions. It is a “hard-wired” system, so the possibilities of configuration are significantly limited.
BIOS is the basic driver for the motherboard. It is a set of primary instructions that are necessary for the computer to run a specific operating system such as DOS, Linux or Windows. Moreover, it influences the performance and the stability. If BIOS is damaged, computer is unfunctional.
“BIOS” of the human brain is represented by a basic program that is responsible for the regulation of the so-called vital functions:
Regulation of the body temperature – centre of thermoregulation is situated in the diencephalon (hypothalamus);
It involves the constriction and dilation of the skin vessels – regulation of the blood pressure and pulse;
Regulation of respiratory functions – the respiratory centre is located in the medulla oblongata and pons;
The program is formed within the first weeks of intrauterine life. Similarly as with computer BIOS, it is “hard-wired” and cannot in actuality be changed. As in computers, it influences “the performance and the stability” of the operation of the human body. Function of the human BIOS is a precondition for running of the “operating program of motor skills” and as with the computer, if the program regulating the vital functions was damaged, the human individual would die as well.
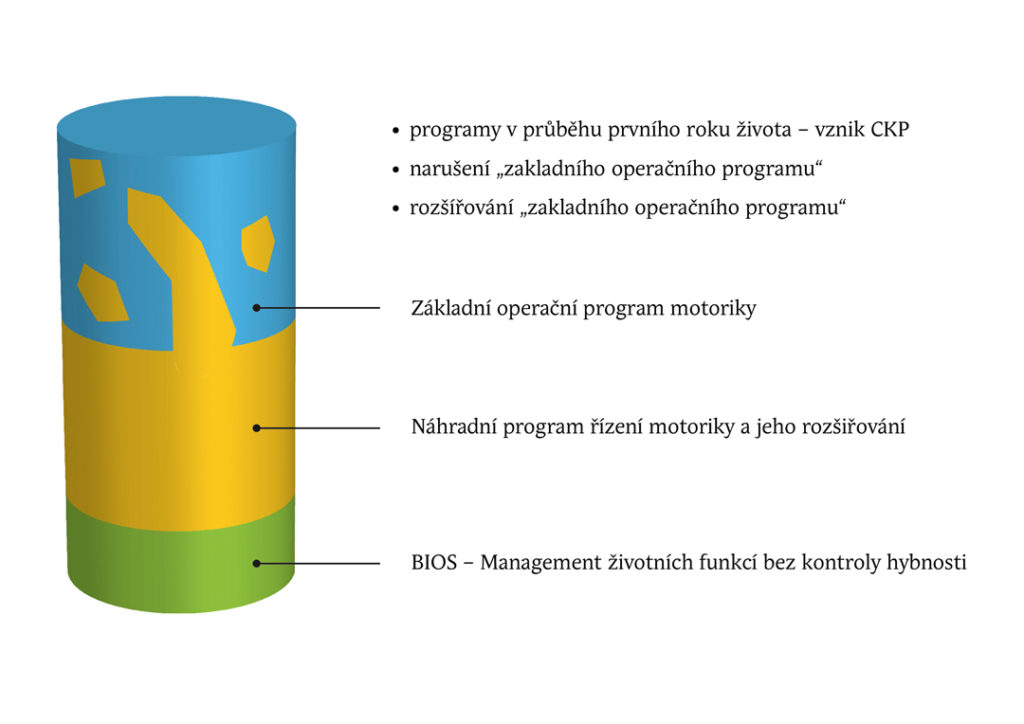
The next layer of regulation that influences the motor skills of the musculoskeletal apparatus is the “Basic operating program of motor skills”.
The program that is fully responsible for the regulation of the basics of our motor skills is the basic operating program of motor skills.
Again, for better comprehension, we would borrow the analogy from the world of computers.
The operating system represents the essential software equipment of every computer. This software runs all technical parts of the computer and provides operational environment for other programs.
Simply put, the operating system collects and controls every operation. If it didn’t, every application would have to perform these activities alone and that would lead to many difficulties (hard drive storing – the files could be overwritten, etc.). Operating system starts with the computer and stays active until the computer is switched off.
It consists of the core and accessory system tools. The main goal of the operating system is to provide the user with the possibility to control the computer, to establish stable application interface and supply the applications with system resources. The operating system is a very complex piece of software. Its development is more complex and difficult compared to the development of ordinary programs.
The best known operating programs are Windows, MAC-OC, LINUX, ANDROID and the older DOS.
Similar construction and function could be found within the basic operating program of motor skills.
We can find the “program core” responsible for the regulation of the basics of motor skills. These contain several necessary building blocks, without which the normal motor skills wouldn’t get by. Creation of these functions on the somatic level, i.e. the myelination, establishment of neural connections, building of neuronal networks and the creation of “virtual maps” take place at the level of genetically determined information without a conscious or targeted learning process – only through maturation.
-
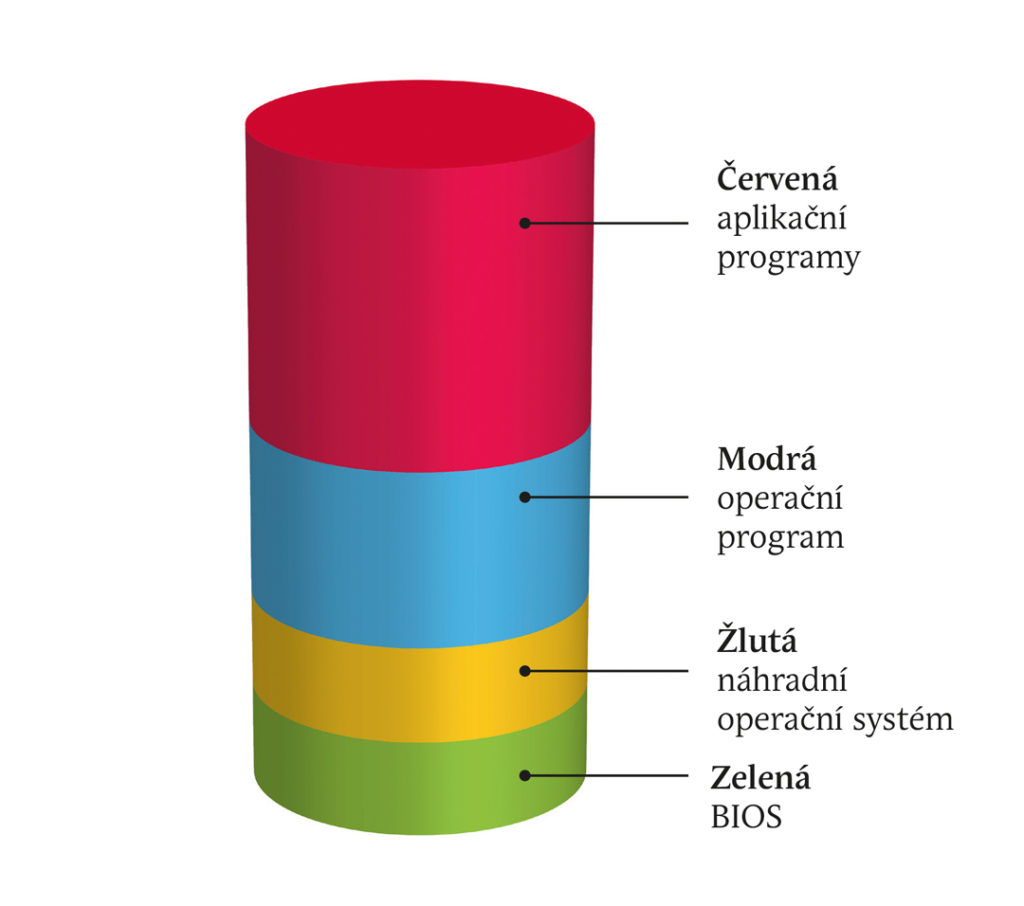
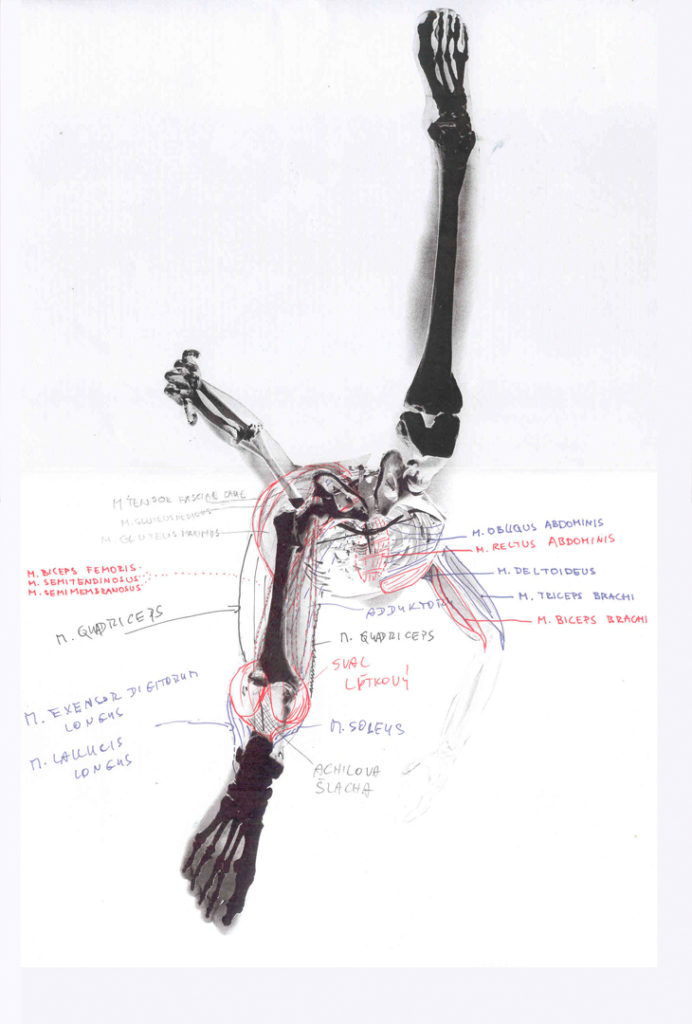
Figure of ideal distribution and tuning of all programs enabling the performance of the most complex motor skills, e.g. ballet.
The human operating system has the following tasks:
I. Autonomic regulation of the posture of the body that has “sub-programs” for management of:
- Autonomic regulation of the resting muscle tone
- Autonomic regulation of the resting muscle coordination
- These two programs create the autonomic regulation of the resting joint centration.
II. Autonomic regulation of the basic stereotypical movements that has the “sub-programs” for control of:
- Autonomic regulation of antigravity and righting programs
- Autonomic regulation of the balance programs
- Autonomic regulation of the coordination of the muscle tone during the movement
- Autonomic regulation of the muscle coordination during the movement
- Autonomic regulation of the joint centration during the movement
III. Original basic stereotypical movements, which follow:
- Autonomic regulation of the stereotypical gait
- Autonomic regulation of the stereotypical grip
- Autonomic regulation of the stereotypical breathing
- Autonomic regulation of the stereotypical swallowing
- Autonomic regulation of the stereotypical ocular movements.
Like the computer operating system (OS), the human OS has got its “auxiliary system tools” that enable and simplify the running and continuous debugging of the “application programs”.
The operating system of human motor skills is extremely complex, vast and genetically determined for locomotion. And this very vastness requires a period of the first year to let the brain grow and run the program completely. This program is autonomic and independent of the conscious control. Full and correct saving to the “disc” enables the brain to let the human individual implement the ideal autonomic regulation of the posture of the body and the ideal autonomic regulation of the basic stereotypical movements. These building stones of motor skills constitute the precondition for non-complicated learning of other “extension” programs of the fine and gross motor skills.
Application programs
User or application programs like Word or Excel make the computer work user-friendly.
BIOS and operating system serve to enable the running of some applications and let us work or play with them. There are hundreds of thousands of application programs and the number is rising.
Similarly, the programs of human motor skills have their application programs. They are not innate. We acquire them by learning. Motor learning enables a very rich range of motion of our body. Within the gross motor skills, we can learn many sport activities like throwing, jumping, hitting, kicking etc.
Within the fine motor skills, the range of abilities is even richer – from writing, drawing, painting and fine arts in general to playing very difficult musical instruments. Fine motor skills of the orofacial region enable speech, singing, and playing wind instruments. All these application programs of human motor skills could be further improved by education and maintained up to old age.
Yet, there is another significant similarity to computer programs. The quality of “the running” of the application programs is utterly dependent on the flawless function of BIOS and the operating system particularly.
If the operating system of the motor skills of the musculoskeletal apparatus was disturbed anyhow, the learning abilities and the running of any application program would be significantly reduced or completely disabled.
Thus, it is absolutely essential for the quality of human life to have “well-tuned” and flawless operating system.
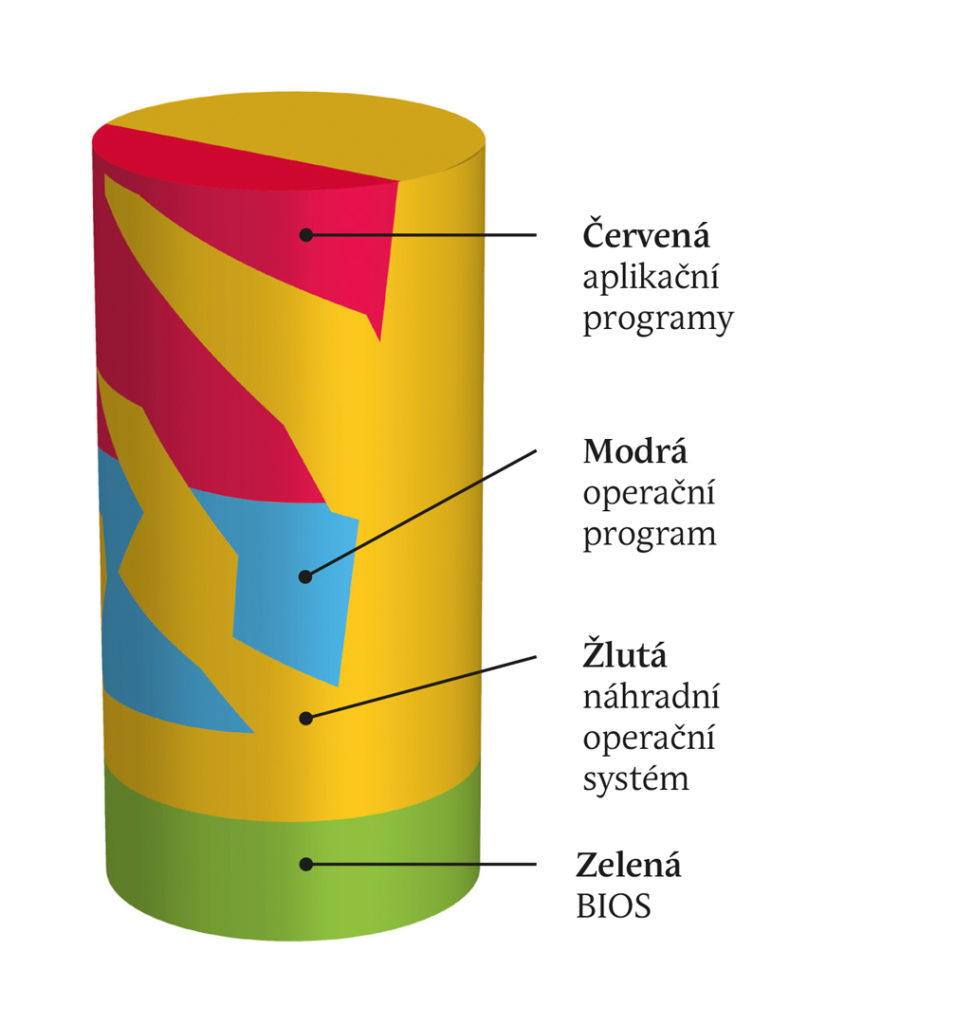
Now, we have reached a program that doesn’t have any direct parallel within the computer world. It is a program we call the substitute operating system.
Substitute Operating System – Trend Towards Pathology of Locomotion
During the normal course of the motor development, the substitute operating system occurs only in traces during the first three months. This is a period of so-called “holokinetic motor skills”. The infant reacts to stimuli with uncoordinated movements of all limbs. Regulation performed by this program is chaotic. If the “unpacking and launching” of the operating system went well, the substitute system would be switched off and it wouldn’t be apparent in the motor skills of the child at about six months of age.
It is kind of a “backup operating program” intended for emergencies, when the operating system has been damaged for some reason. Hence, the substitute program is loaded and launched to an extent corresponding with the damage of the operating system. It could be used only for the control of one limb or of the whole body. A substitute program serves to maintain life. To run the application programs could be significantly more difficult with it or even entirely impossible, no matter if it were the programs of fine or gross motor skills.
-
Depiction of a common situation: the substitute system is not completely “switched off” and interferes with the regulation of the operating system (impairs the autonomic regulation of the posture of the body) and interferes with application programs and restricts their activity.
There is certain analogy from the world of computers in comparing the current operating systems with the first primitive operating systems like MS DOS. It had no graphical interface and the regimen was based on the user environment represented by a command line – it was simply impossible to click on the icon of a file we wanted to run. Also, it wasn’t possible to run the application so simply. Commands the computer was supposed to perform had to be written in the command line. The commands were combinations of letters and numerals. The essential insufficiency of the DOS program is that the 3D movement of the pelvis against the chest is impossible.
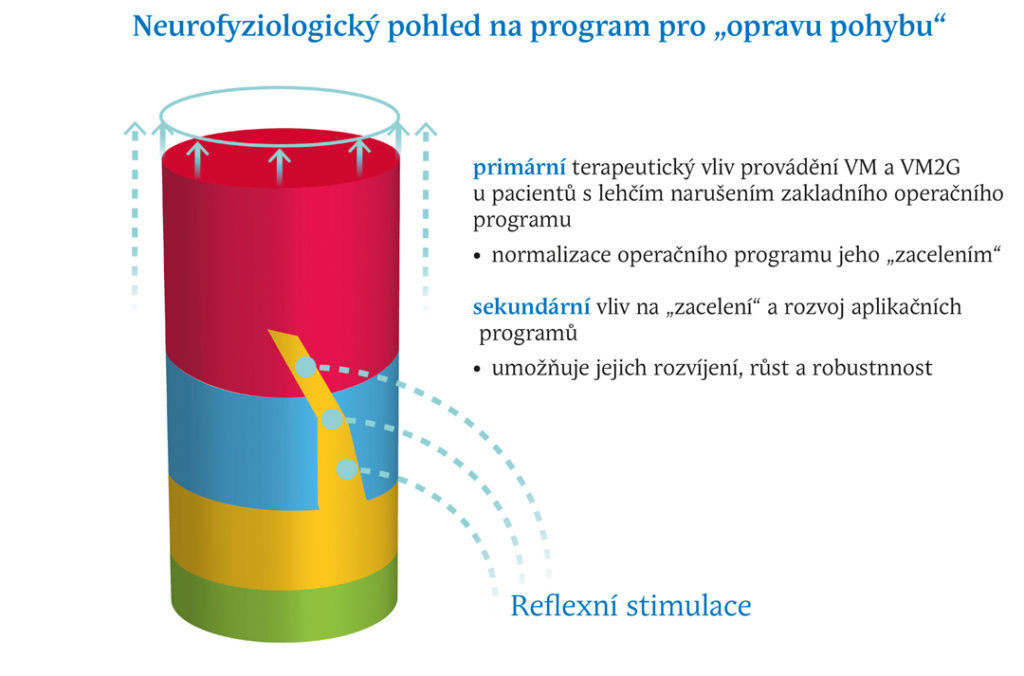
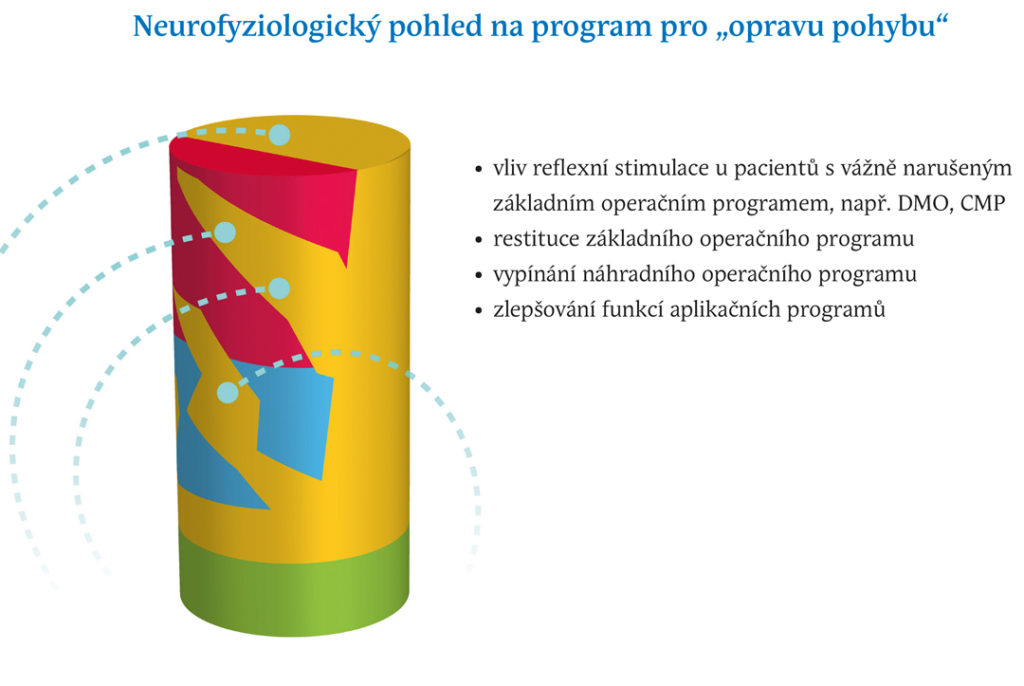
Neurophysiological view of the program for “repair of locomotion”
From a clinical point of view, the individual levels of regulation of the nervous system could be evaluated as follows:
The level of the higher nervous activity that contains the general intelligence, specific motor intelligence, voluntary processes, motivational and instinctive processes, emotional processes, memory processes of remembering and reminding and gnostic functions.
The level of application programs of fine motor skills including oculomotor skills (reading, watching a movie…), phonation motor skills (speech, singing…), facial gestures and orofacial region motor skills and the lingual motor skills (speech, singing, facial expression), motor skills of the hand and fingers (writing, painting, playing the musical instruments…).
Level of application programs of gross motor skills, e.g. sports, gymnastics, manual working habits, common acting abilities, “bodywork”, etc.
Level of basic operating system of motor skills containing the basic stereotypical gait, basic stereotypical grip, autonomic righting and postural reflexes (postural reactivity), autonomic posture of the body, basic stereotypical respiratory mechanics, stereotypical swallowing and defecation.
-
Depiction of a situation of a severe impairment of the operating system, which is largely completed with the substitute program
Level of substitute operating system of motor skills that enables basal survival with substitute stereotypical movements for the stereotypical gait, stereotypical grip, autonomic righting and postural reflexes (postural reactivity), autonomic posture of the body, autonomic respiratory mechanics and autonomic stereotypical swallowing and defecation.
Level of regulation of basal vegetative functions at the level of the brainstem – “BIOS”. Cardiopulmonary functions, haemodynamics, regulation of basal metabolism, protective reflexes (cough, sneezing, corneal reflex…).
Repair program
It seems that BIOS contains something like a “program cluster”, which is inactive under common circumstances. If its activation was performed in a completely specific way, it could be used as a “repair program” that can reconstruct the basic operating program of motor skills. The only known way of such activation is the Vojta methodology of reflex locomotion. I imagine that the repair is implemented by the repair program, which adds the missing “information library” to the undeveloped (“unzipped”) operating program. Under physiological circumstances, the OS is loaded during the first year of the ontogenetic development.
Another type of repair could be utilised for damages that have developed in older age despite the aetiology of the impairment.
This specific repair cluster probably contains complete information on the basic operating program of motor skills of the human body in a comprised form. It can be supposed that it also represent “data storage” for “program cores” of application programs and other information from higher nervous activity.
The repaired program in the activated state performs the mapping of the actual condition of the operating program and subsequently, or rather concurrently, it implements the addition of missing “information libraries” and reconstruction or “patching” of the operating program. Concurrently, it performs the complete check-up of the whole musculoskeletal apparatus. “Information files” are stored during the repair process into the cerebral matrix so that they could be used for launching and running of the autonomic regulation of the posture of the body, postural reactivity and autonomic stereotypical gait, grip and other stereotypical movements.
Subsequently, it enables the running of the extension application programs including the programs of higher nervous activity. The clinical launching of the repair program itself is only known through the activation by reflex locomotion (reflex turning, reflex belly-crawling and reflex crawling on all fours).
This activation could be divided to the system of “locks” and “keys”.
A system of locks contains the defined positions of the body (of the axial organ and limbs), position of the body in the gravitational field, supporting points or more or less exactly defined supporting surfaces and supporting lines as the case may be.
A system of keys contains the stimulation of defined activation points and zones, the ways of stimulation of these points and zones by pressure, pulling, vibrations in defined vectors and combinations of these activation points and zones and stimulation vectors.
Only if the system of “locks and keys” starts to fit together, the repair program would be activated. During the very “running” of the repair program, the “application programs” of fine and gross motor skills are completely switched off. The centres of higher nervous activity are also gradually “switched off”. Conscious processes are inhibited into the relaxed state to the limits of the transition from the conscious state to sleep. Gradually, the centres of conscious proprioception and kinaesthesia switch off to the limits, where the bodily scheme ceases to be perceived.
Activation of the repair program through VM reflex locomotion is completely independent of the function of the higher nervous activity. It is obvious during the therapy of children under one year of age and patients in vigil coma.
Videa – Míša 1. a 2. cvičení
The very operating program of motor skills is also utilised during the stimulation by reflex locomotion. All his parts are activated, i.e. the autonomic regulation of the posture of the body, postural reactivity, stereotypical gait, stereotypical grip, stereotypical breathing, stereotypical swallowing and defecation. But all these mechanisms take place in the substitute “economic” mode.
Case Study – Daniel Pulled out of the Lions’ Den

Illustration of the Therapy of the Severe Congenital Developmental Defect of the Brain
Daniel is the third child of our friends Olga and Mirek. We had known them for many years, and both of their older daughters were in my care. I examined little Daniel at five weeks of age. The results of the examination proved the fears of his parents that there wasn’t something right with him. One side of the body showed significant pathological asymmetries in all positions, particularly in the positional tests. Hence, we started the therapy very early. Despite the early commencement of therapy and the intensive home implementation, the lateral asymmetry didn’t improve. In his six months of age, Daniel was sent by the paediatrician for neurological examination, which recommended the examination with magnetic resonance imaging. Daniel went through it in the twelfth month of life. The result was even worse than expected. The description of the magnetic resonance imaging of the brain showed that there was a cortical dysplasia of the right hemisphere with impaired gyrification (pachygyria) and there was also partial widening of the lateral cerebral ventricles. Subsequently, consultation description of the MRI was made in IKEM hospital. It showed even larger impairment. Practically, the whole right hemisphere was affected, particularly its “outer” region (the convexity) of the frontal, parietal and temporal lobe, with an exception of the occipital lobe. Concurrently, according to age, they described retarded myelination of the white matter diffusely in the brain. Among others, the diagnosis was set: “Insufficient presumed normal physiological development of the nervous system – left-sided hemiparesis”, i. e. cerebral palsy of the left side of the body.

Clinical Description of the Problem
Brain dysplasia, more recently referred to as malformations of cortical development, is the congenital developmental defect of the brain that originates in the early stages of embryogenesis. This term predominantly describes the disorders of migration and neuronal differentiation. Pachygyria, i.e. excessive thickening of the cerebral gyri, is among the disorders of cell migration and organisation of the cerebral cortex with reduction in the grooves of the cerebral cortex. Approximately 3 % of new-born children are affected by this congenital developmental defect. This count also represents the congenital developmental defects of the brain. Concurrently, these congenital developmental defects, cerebral dysplasia in the strict sense, are often combined with the development of epilepsy and psychomotor retardation. The development of the nervous system is a very complex process, which connects the morphological and functional changes together. Normal development of the individual is dependent on its perfect course. The development is genetically determined by several regulatory genes that encode regulation proteins. Their function consists in stimulating stem cells to proliferate.
Cerebra dysplasia is quite often connected with development of epileptic seizures from the new-born and infant age. (This is relevant predominantly in diffuse disorders of migration that affect large brain areas.) The infants usually develop the seizures presented with flection spasms. Concurrently, the psychomotor development stagnates. In old age, partial seizures caused by the focal cortical dysplasia appear. Pharmacological resistance is common in cerebral dysplasia. Depending on the localisation and extent, cerebral dysplasia relates to various neurological findings (central palsies of cerebral nerves, central hemiparesis in schizencephalia, mental deficit and retardation of the psychomotor development expressed to various extents).
Expert Explanation of the Problem
In Daniel’s case, the almost typical development of cerebral palsy could be expected due to clear causes. Undoubtedly proven brain damage caused by the congenital developmental defect would explain the further unfavourable development. It would head towards the symptoms of the hemiparetic type of cerebral palsy with highly probable development of epilepsy and mental deterioration.
Illustration of the Solution
Intensive therapy had been implemented with Daniel since the fifth week of life for five times a day. In the first six months, Daniel’s mother could manage the exercises by herself. She and Mirek took turns. Later it was necessary that both were present during the exercise. The training intensified due to the use of a special “training suit” and later of the paediatric rehabilitative bed, and other tools like antiskid mats, lability balls, discs and weights were used. Thanks to these aids, the very exercise was more comfortable and more intensive. Olga and Mirek could evaluate the change in exercise very well as they were experienced because of their daughters’ exercise without these aids. This intensive therapy lasted for almost two years. For a long time, it seemed that nothing was happening. Daniel’s development shifted forward by almost imperceptible steps, and there were periods of no progress at all. At thirteen months of age, Daniel didn’t crawl; he turned around only to one side; he didn’t use his left hand as if he didn’t know about it. The left lower limb was as though “dead”. At about two years of age, Daniel started to get on his knees. Initially he moved forward by hopping and after two following months, alternate crawling appeared. Still, the supporting function of the left hand was significantly reduced. At that time, the intensity of exercises decreased to three times a day with free Sundays. It was a great relief, because both parents were at their wits’ end. At two years and four months, Daniel stood up; his first steps started by holding his hand. Over the following two months, Daniel began to walk on his own. His left hand has gradually regained its function, while it was neglected by Daniel for a long time. He hasn’t yet used it to grip something.
Explanation of the Solution
The fact that the VM2G therapy began very early after Daniel’s birth appeared to be extremely important. Equally, the intensity of the stimulation has been very intensive since the very beginning of the therapy. This has played a key role during the whole process of normalising of the psychomotor development and it has prevented the expected onset of spontaneous brain pulses, i.e. epilepsy. Epileptic seizures significantly worsen the “condition” of the brain and disrupt the reparative processes stimulated by the therapy. Despite the continuous diagnostic results, the expected diagnosis – a lack of, presumed normal physiological development of the nervous system – left-sided hemiparesis – wasn’t accomplished. Following the early diagnosis, based on its results, maximal frequency of the performed stimulation has been chosen since the fifth week, i.e. five times a day. Each exercise took thirty-five to forty minutes. After sixth months, both parents participated in most exercises. The stimulation technique was gradually intensified by a special training suit that provided multizonal stimulation. In Daniel’s case, there were 21 specifically chosen zones.
The use of the children’s rehabilitative table, which allows the performance of VM2G on tilted surfaces, meant another intensification of the stimulation and it happened to significantly enable the implementation of the therapy by parents. Other aids played appreciable role as well – the antiskid mats, labilising discs and balls and limb weights. The goal of this extremely intensive, long-lasting, technically demanding stimulation was to lead Daniel from the realistic and severe threat of congenital developmental defect of the brain – literally, to pull him out of the lions’ den. This threat was imminent for more than 2 years. Existing clinical experience shows that these types of congenital defects lead to extremely severe and lifelong handicaps in terms of DMO, epilepsy and mental retardation. We think that the only intensive and higher than average endeavour and self-sacrifice of the parents prevented the pathological development. Only after sixteen months of therapy, the physiological motor development began to accelerate significantly. Bilateral turning occurred followed by righting and crawling on all fours. At the age of two and half, Daniel began to walk. The gait gradually became unaided, balanced and matured in terms of the stereotypical movement. Recently, Daniel has gradually accomplished the therapy, so that he could fully utilise the functions of the left hand. The hand has normal posture without pathological features, with normal joint centration, but it hasn’t been completely included into the basic stereotypical grip.

The View of the Possibilities of the Advancement of Motor and Mental Functions in Terms of VM2G in Infant Patients with Congenital Developmental Defects of the Brain with Confirmed Severe Neurological Findings and Very Severe Prognosis Concerning the Upcoming Development
In terms of VM2G, it was revealing that in such severe cases, the course of the therapy is quite different from common “standard” central coordination disorders, even the severe ones. These differences could be seen within the long-term and torpid persistence of primitive reflexes, which prevent the normal physiological development despite the massive therapeutic stimulation. On the other hand, there is still further good news – the stimulations could seem ineffective for several months. The therapy stays in a state of arrested development. It doesn’t head in a pathological or physiological direction. In terms of developmental kinesiology, this “static period” is essential because this stagnating phase means that the expected onset of pathological motor skills does not appear. Otherwise, they would inevitably start and would gradually rule over the motor skills of the child after the first year of life, resulting in the definitive stage of some type of cerebral palsy with concurrent epilepsy and mental retardation. It’s the phase of stagnation when an intensive therapeutic fight takes place to prevent the pathological course. From the outside, it looks like falling behind. Only after the intensive therapy has set normal conditions in the cerebral matrix probably because of concentration of the neuronal matrix and reaching sufficient “transmission capacity” of the afferent and efferent neural pathways, the normal physiological development could be implemented. It appears in the complete elimination of the primitive reflexes and particularly in the onset of the totally physiological development within its natural phases. This could utterly prevent the development of substitute pathological posture of the body and limbs and the subsequent features of substitute stereotypical movements. I think that the therapeutic stimulation has used the cerebral plasticity that is extraordinary within the early stages. The probable factor explaining the ability of new neuronal formation would be the mechanism of neurotransmitters, which probably initiate the activation of “dormant” stem cells. This launching mechanism would probably explain the primary therapeutic effect of VM2G. It seems that the intensive and long-term brain stimulation is probably the only possible way to secure the neurogenesis, which has been disturbed. The distortion of the normal development of brain tissue relates to another gradual cascading deterioration in time caused by genetically determined apoptosis. Neurons that couldn’t be connected into the neuronal networks due to inactivity or hypoactivity are mostly affected by this process of programmed death. Premature utilisation of immature neurons contributes to deterioration of the neurological symptoms. Thanks to insufficient differentiation, these neurons cannot fulfil their expected functional responses within the operation of neuronal networks. This increases the overall havoc in the brain function. This functional and even anatomical chaos is undoubtedly the “breeding ground” for the development of global chaotic discharges, i.e. epilepsy.
Concurrently, these damaged processes of maturation of cerebral tissue are the precondition for persistence of primitive new-born and infant reflexes. This prevents the onset of physiological developmental programs of righting and locomotion. Thus, the gradual development of substitute pathological motor skills evolves.
Dr. Vojta states on the page 350 in the last chapter of his best-known book Cerebral Motor Disorders of the Infant Age,:
“There is a certain rule: If a year-long intensive treatment of a child with CP does not show any significant improvement, we must admit, we’ve reached the limits of the possibilities of our therapy. To make such a conclusion naturally requires great experience and knowledge from the physicians and rehabilitative workers.”
The experience we have gained with VM2G therapeutic approach reaches beyond these limits.
Byrtus Daniel
Byrtus Daniel