People were created for beauty. This could be read in the biblical book “Song of Songs”, which extols the beauty of the woman and the man.
“Your teeth are like a flock of shorn ewes that have come up from the washing, all of which bear twins, and not one among them has lost its young…. Your neck is like the tower of David, built in rows of stone; on it hang a thousand shields, all of them shields of warriors…. His arms are rods of gold, set with jewels… His posture is stately, like the noble cedars of Lebanon.”
This and many other books describe the beauty of the perfectly matured human body that underwent the flawless development of the locomotive apparatus. In clinical terms, we could say that such body has ideal poise, i.e. ideal posture, and that the basic stereotypical movements are perfectly balanced and coordinated.
The excellent condition of the musculoskeletal apparatus in terms of adequate amount of muscle and fat tissue and symmetry of the composition of “bodily masses” would be the third aspect.
All these aspects, if balanced between each other in an adequate ratio, create the preconditions for the true beauty of the female and male body: a charm that needn’t be further glamourized.
Many have tried to depict this beauty artistically since ancient times. It seems that renaissance genius artists Leonardo da Vinci, Michelangelo Buonarotti and Sandro Botticelli truly reached the peak. They understood that beauty is tightly bound to the functionality of the body. Thus, they precisely researched and described the anatomy of the human body. Without any doubt, pieces of art that have come from this knowledge represent the best of fine arts ever created.
This book also tries to translate the knowledge and experience that represent the way of healing the musculoskeletal apparatus. Reattainment of beauty and dignity of the human body is related to that.
A female patient convinced me of the important relation of the posture and movement of the body to its charms. She not only wanted to get rid of her back problems; she also wanted to walk elegantly in high heels. She has had problems with walking on high heels as the tips of her feet tended to turn inwards.
As will be presented later in this book, in terms of developmental kinesiology, inner rotation of the feet and turning the tips of the feet inwards is closely related to problems in the spinal region. Six months of therapy removed the back pain and enabled her to walk in high heels without any problems. Thus, it led to normalisation of her stereotypical gait. The high efficacy of this intervention that led to the beauty and smoothness of motion is a very favourable result. In the upcoming chapters, in the examples of several case studies, we can see for ourselves the results of the therapy that has led to usefulness and beauty.
VM2G as the Direction Towards Locomotion
We have been programmed for locomotion. In general, we can say that the more perfect the locomotion gets, the better lived life itself can be.
-

Before the therapy
-

After one year of the therapy
-
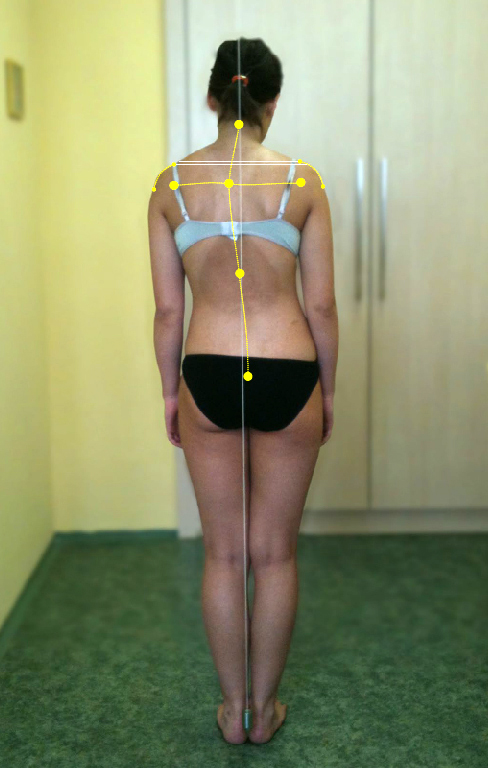
Before the therapy
-

After one year of the therapy
VM2G uses our own given and unchangeable genetic programming for locomotion. It’s the innate genetic program with which the VM2G “works”. It uses the program for therapeutic purposes. It’s a program that has been intended to lead us after birth to the upright autonomic posture of the body against gravity and has enabled the a bipedal gait. This allowed the upper extremities to become specialised for grasping and manipulating objects. When this program reaches its target usually at about one year of age, it switches off automatically. It’s useless as we begin to use the possibilities of the autonomic bodily posture and autonomic movement stereotypes.
VM2G works as the therapy that stands on the possibilities of changes of the mutual relationships of individual systems and organ systems of the human body.
Revoking the genetically determined motor program is the relevant process that happens during the implementation of the classical Vojta method and VM2G as well. This happens via the reflexive path through mechanical irritation of the reflex zones of the body. This process resembles the stimulus of the simple reflexes during the neurological examination, e.g., the patellar reflex. These simple reflexes are regulated at the spinal level and are also induced by a mechanical stimulus, most often through gently striking the relevant place on the body. The response to stimulation, which is easy to see, consists in prompt contraction of the respective muscle group and the subsequent immediate relaxation.
The global reflex, which has been used in the Vojta method, is regulated by cerebral structures, although it surely uses the spinal mechanisms too. The region at the centre of regulation of the global reflex is not known exactly. While it can be induced in patients in coma, we can presume that it is localised in the subcortical brain structures. The response is not the immediate contraction and subsequent relaxation of the muscles as in cases of simple reflexes. It is the slow connection of individual muscle groups into muscular chains. The resulting movement depends on the main muscular chains, which we have just induced in the reflex way. Which muscular chain is activated as a main one totally depends on the position of the body of the patient. It would determine the course of the reflex movement.
The basic “starting” setup positioning of the body is a necessary precondition for stimulating the global reflex. These “starting” positions are also necessary for stimulating single reflexes, e.g. we would hardly induce the patellar reflex in standing patient.
What Is Not VM2G
This is not an active exercise, during which we would try to change the actual status of the musculoskeletal apparatus with conscious effort. It’s not an effort to change the current muscular length of individual muscles or muscle groups such as in stretching or yoga exercises. VM2G is not an active increase in strength of chosen muscles and muscle groups that takes place in bodybuilding and strengthening techniques.
Case Study – The Implementation of the VM2G in the Therapy of Severe Peripheral Palsies.
Illustration of the Solution of the Postpartum Brachial Palsy
Monika was the youngest patient taken into our care. She was only 3 days old, when her mother brought her. The delivery went awry. The mother suffered a coccygeal fracture. When the delivery didn’t go well, the obstetrician pulled the head with too much force. Thus, there was a complete palsy of the whole upper limb of the new-born from the scapula to the hand. The first neurological examination in the maternity hospital indicated that the condition was severe. The whole limb didn’t show any movements and there were no responses to external stimulation. The mother was well informed about the risks of unfavourable development of the upper limb. She started the rehabilitative care with great zeal as she knew she was fighting for her daughter’s future.

Description of the Problem (Clinical Findings)
A detailed history including the description of the delivery confirmed that there was complete brachial palsy of the upper and lower type. The traumatic manoeuvre injured the innervation of the muscles of the scapula, shoulder and arm, as well as the forearm and the whole hand. The muscles were completely hypotonic including the reflex joint hypermobility. It was necessary to be extremely careful during the treatment in order to prevent secondary trauma to the totally plegic limb. The efforts to induce any kind of neurological reflex on the affected limb were completely useless. A neurological report suspected the interruption of the brachial plexus root nerves as highly probable. The impairment of sensitive innervation was visible in the marble-coloured skin and the mild swelling of the whole limb. Motor functions of other limbs were completely normal. CNS function also did not show any impairment.
Expert Explanation of the Problem
Postpartum paresis of the upper limb represents extreme psychological and also subsequently physical stress for the mother of the injured new-born. The mechanism of the injury consists in the pulling of the head of the child stuck in the birth canal. The child’s stuck shoulder results in stretching or partial to complete rupture of the root nerves of the brachial plexus. The disorder is usually represented by the upper type of palsy that affects the nerves innervating muscles of scapula, shoulder and arm. Lower type of palsy is less common. It affects the nerves innervating the muscles of the forearm and the hand. If both types of palsy occur concurrently, severe damage to nerve plexus could be suspected. There is usually stretching or partial to complete laceration of the root nerves. The prognosis of this condition is very severe. Without early, intensive and properly guided therapy that would use the regeneration potential of the nervous tissue, the future basal motion and primary functions of the whole arm and hand would be critically threatened. Early muscular denervation and subsequent irreversible morphological and functional changes in the muscles would develop, unless the intensive but adequate stimulation did use the possibilities of early regeneration of the nervous tissue. Insufficient innervation causes the remaining peripheral neural connections to fall under the influence of neural inhibition. Subsequently, the neural alienation would spread at the level of the central regulation. Hence, the whole affected limb misses out on any connection, i.e. regulation. In terms of developmental kinesiology, the dysfunctional upper limb entails great restriction for the development of the musculoskeletal apparatus. It is forced to search for substitute movement mechanisms that would replace the missing limb. The limb is eliminated from the kinetic muscular chains and the biomechanical bonds are impaired. This disturbed development might lead to significant muscular coordination imbalance in adolescence that could end with scoliosis of the spine or the ribcage deformity. If the therapeutic effort was meant to be effective, it would have to be aware of all these above-mentioned aspects. Intensive stimulation of the paretic nerves is extremely difficult. If it was performed consciously, it would easily lead to overload with a need subsequently for long regeneration. Stimulation implemented regarding the principles of the genetically determined motor programs bypasses this problem without any fear. The innate programs themselves have the feedback protection implemented. It would not permit the paretic muscles and nerves to become overloaded. These control mechanisms are reliable and tested by a longstanding practice. The other problem with the exercise of the paretic muscles under conscious effort is the development of synkineses. They disturb the very movement because the muscles, which are denervated less than others, join in movements, which they shouldn’t. This problem is not known in reflex stimulation because the repair reflex programs predetermine coordinated stimulation, which wouldn’t allow the development of synkineses. The third severe complication of analytical stimulation of paretic muscles is their incorrect connection into the muscular kinetic chains and the stereotypical movements. Reflex stimulation works within the basic stereotypical movement and would not permit any part of the locomotive apparatus to contribute to the kinetic stereotypes incorrectly. In the Czech Republic, the treatment of the postpartum brachial plexus palsy with the Vojta method is now obligatory. Our experience using VM2G seem to be very successful even in the most severe types of these injuries.
During the first year of age, the use of the Vojta method is relatively easy to perform, as the changes occur at the time of the child’s unaided standing and walking. Due to the maturation of basic motor programs, the child has the possibility to disturb the induction of the stimulatory reflex. The option of rational agreement with the child of one to five years of age is quite restricted. That’s why the Vojta method is usually finished and the parents are usually advised to stimulate the affected hand by putting the toys in it. This advice is a result of not understanding the conditions and abilities of the neurophysiological situation and the level of the mental maturation of the child. It is an unacknowledged fact that the child hasn’t developed the stereognosis in the affected hand yet. The toy couldn’t properly be recognised by touch. Thus, there is no chance of attracting the child’s attention with it. If the motor function of the affected hand didn’t fully normalise during the first year of age (which is rare in cases of combined upper and lower type of palsy), the continuation of the therapy with reflex stimulation would be necessary. The approach must respect the status of the child’s mental development.
Illustration of the Solution
The very implementation of the therapy was extremely difficult. Right from the beginning, it was necessary to start with the reflex stimulation by VM2G four times a day. In the first year, the check-up visits took place once a week. When the patient was six months of age, the more demanding kind of stimulation had to proceed. It was performed at home by the mother and another person. The second assisting therapist was the patient’s grandmother, but for a certain period she had to be replaced by the aunt or a helpful neighbour from their block of flats. The influence of the intensive stimulation led to the gradual connection of the muscles in both the upper and lower parts of the limb. That’s why the motor development could run normally during the first year. The hand gradually contributed to the normal stereotypical movements of turning, stabilisation on the side, grasping, crawling, support during standing on all fours, crawling on all fours and finally in the stereotypical gait. Since the time of unaided walking, it had been necessary to change the training approach. We started to use far more playful ways of diverting the attention like songs and nursery rhymes. Until three and half years, the exercises were performed twice a day with the help of the second home therapist. Later, the mother alone exercised with the patient once a day. In the next year, when the mother became pregnant, we tried to find a way to continue with Monika’s exercises. The home exercises were quite physically demanding at that time and it was basically impracticable for the pregnant mother. The solution was found in the new conception of the implementation of VM2G with help from a home therapist. Little Monika quickly became fond of her “auntie Dáša” – the home therapist and the exercises continued very well. Little Monika has the right degree of respect and stopped to use her “tricks” to shorten the exercises as she had tried with her mother. The use of training clothes implemented another intensification of therapy and fun for Monika. Due to the proper and intensive therapy, the consequences of this very severe perinatal trauma almost normalised. The motion of the whole shoulder girdle and in the elbow was restored, and the hand is as adroit as the other. The stereotypical movements are normal. The only remaining problem to treat is an insufficient stability of the arm during the outer rotation.
Explanation of the Solution
The course of the therapy and the recent result could indeed be considered as acceptable. The initial highly uncertain prognosis of the future function of the hand quickly changed to assurance that the arm and hand wouldn’t remain plegic and non-functioning. Severe trauma of the peripheral nerves requires the fastest commencement of therapy possible, which must be intensive and with the proper aims. The performance of VM2G enabled the start of the permanent maintenance of the reparative processes. The very process of neurogenesis and the inhibition of central alienation constitute the target of the stimulation. Due to use of genetically determined motor programs, it is possible to perform the stimulation with maximum efficacy without risk of overload. Feedback, which happens automatically in reflex stimulation, enables an amount of the stimulation that is practically independent on the external conditions. If the control system identified a potential overload, the stimulation switches off automatically. Its next activation is enabled when the nervous system regenerates and gets ready to endure the next stimulation load. The intensity of stimulation was gradually increased by technical aids. As Vojta highlighted, the aids help to increase the spatial stimulation of the stimuli. Temporal stimulation was maximally implemented, in the first year particularly, when the exercises were performed four times every day. All currently used therapeutic aids were implemented, i.e. stimulation balls, antiskid and balance mats, tilting of supporting surfaces and the training dress. In the subsequent years, the concept of using a home therapist was proved useful. She established a kind but uncompromising order during the exercise. This common-sense approach to setting limits was a relief for the whole family. The patient has tolerated the exercises with “auntie” very well without protests or evasive tactics.
The View of the Traumatic Postpartum Brachial Plexus Palsy and Its Solution in Terms of VM2G
VM2G has proved to be very useful in therapy of peripheral palsies of various aetiology, particularly in cases of postpartum brachial plexus palsies. Reflex induced repair programs are extremely effective and completely safe. It’s the safety of the therapy that allows us to put the practical implementation into the hands of parents and home therapists. There is a remaining precondition of the leadership and supervision of the VM2G by an experienced physiotherapist. In the peripheral palsy, the functional impairment quite quickly spreads towards the morphological impairment. These functional and morphological impairments start to manifest in functions of other parts of the locomotive apparatus. Disconnection of the affected limb from the basic stereotypical movements may induce deformities of the ribcage and the spine with the tendency to scoliosis.
Therapeutic intervention of VM2G is manifested in the normalisation of the programs responsible for regulation of motor skills and subsequently in the normalisation of the trophic appearance. The goal is to completely normalise the motion of the affected limb, involve it fully in the stereotypical movements and normalise the whole locomotive apparatus and the autonomic regulation of the posture, including the basic stereotypical movements.
The omission of the therapeutic intervention in children with traumatic brachial plexus palsy would be a source of significant future inhibition of complex development of the personality of the patient. The inhibition would manifest itself in many areas of life, i.e. education, sports and playing musical instruments. It also bears significant social stigma, including future economic activities.
Video – Veselá Monika
Video of the family interview