The ideal development during the first year of age is the essential precondition for keeping a correct posture of the body during adulthood, i.e. according to “the original hard-wired idea” or the genetic plan. If the development was disturbed in any way during this sensitive period, it is very probable that some disorder of the statics or dynamics of the musculoskeletal apparatus would appear in adolescence or adulthood. If the development was accomplished between fifteen and seventeen months of age, it would be obvious whether the musculoskeletal apparatus would be able to tolerate the stress, and eventually, which disorders could be expected to appear.
If the motor development was distorted during the first year of life, the following growth in adolescence would lead to further progression of these disorders. The following care is predominantly rehabilitative and orthopaedic. Luckily, there are only few of these cases in the population (3-5 %). More often, milder developmental disorders occur. Often, they aren’t obvious or they are considered irrelevant due to their supposed minuteness. Then, they aren’t properly treated. Consequently, the results aren’t perfect for the development of the musculoskeletal apparatus and subsequent ossification of the disorders. The disorders of the locomotive system are manifested in terms of “hardware”, i.e. the musculoskeletal apparatus, as well as the regulation of the locomotion of the body, i.e. the “software” disorder of the CNS.
Case Study – Hyperlordotic Posture and the Ventral Posture of the Pelvis (Risk of Development of Scoliosis even in the Case of Small Unevenness of the Pelvic Axes)
Illustration of the Developmental Complications and the Questions Connected with the Development of Spinal Scoliosis (Implementation of Technical Aids – Anti-Slip Mat and Elastic Bands)
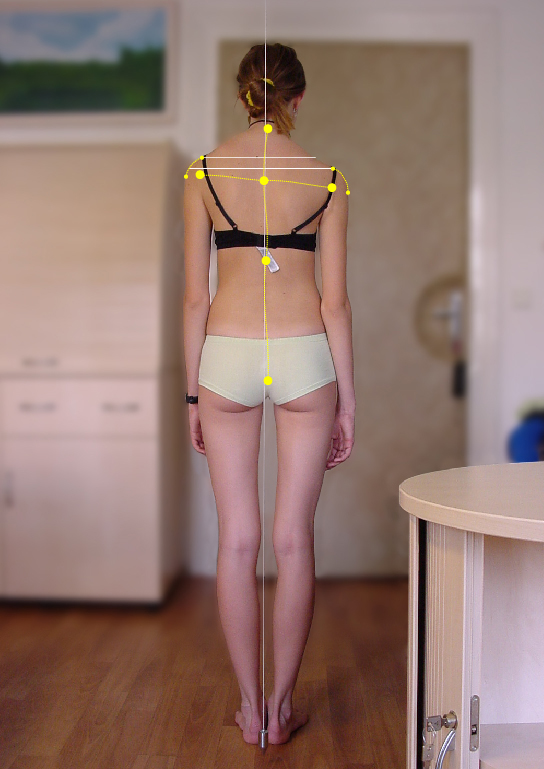
Our treatment was recommended by an orthopaedist to the female patient due to incorrect posture of the body. The asthenic girl came accompanied by her mother that described her daughter’s problem as “incorrect stance”. She explained that she’d tried to convince the daughter to stand nicely. Otherwise, she would develop back pain or scoliosis. The problem stretched back to the time when she had started to walk and had worsened recently. It was obvious in the lateral view with a plumb line. They had attended various rehabilitative exercises without any relevant success. The daughter was physically gifted and her school results were good. The mother was mostly worried about the possible development of scoliosis. Both parents of the patient were tall and slim.
Description of the Problem (Clinical Findings)
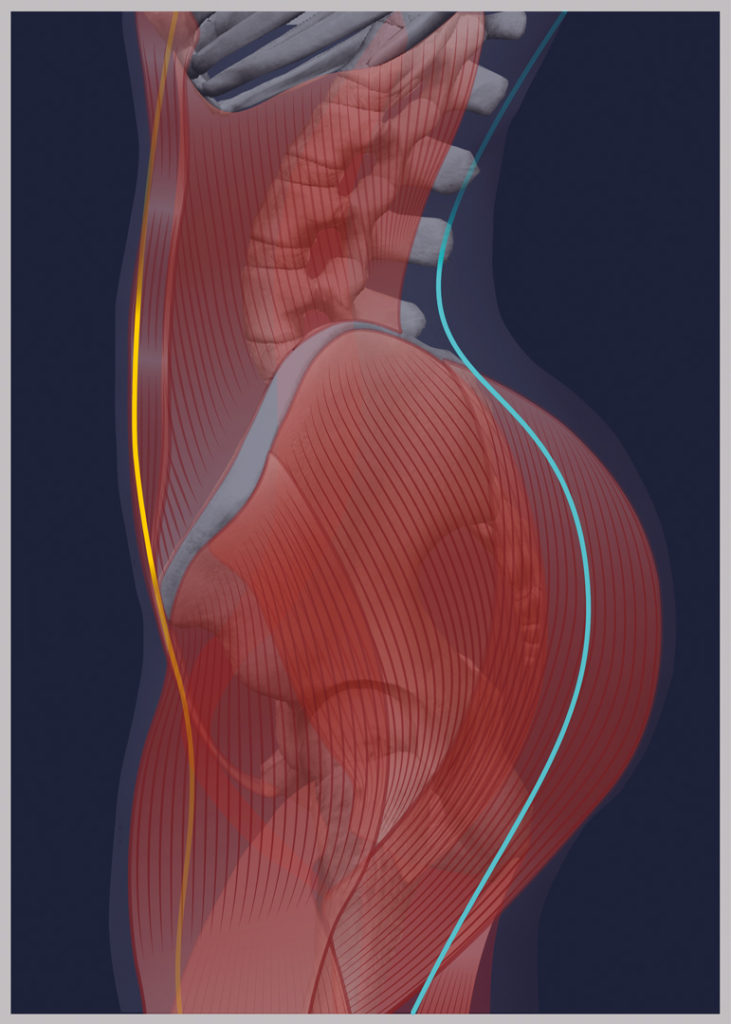
The patient’s history from the first year of life didn’t show anything noteworthy. Only during the second year, impairment of the posture of the body occurred in terms of hyperlordotic posture of the lumbar spine reaching up to the middle parts of the thoracic spine. The rest of the thoracic spine was flattened and missed the kyphotic bending. The abdominal wall was arched and partially relaxed due to the ventral flection of the pelvis. The shoulder girdles protruded forward. Head posture and the posture and configuration of the lower limbs didn’t show any clinical abnormalities.
-
Th e collapse of the arches of the feet, deviations of the axes of the calcanei, tarsal bones and digits - Expert Explanation of the Problem
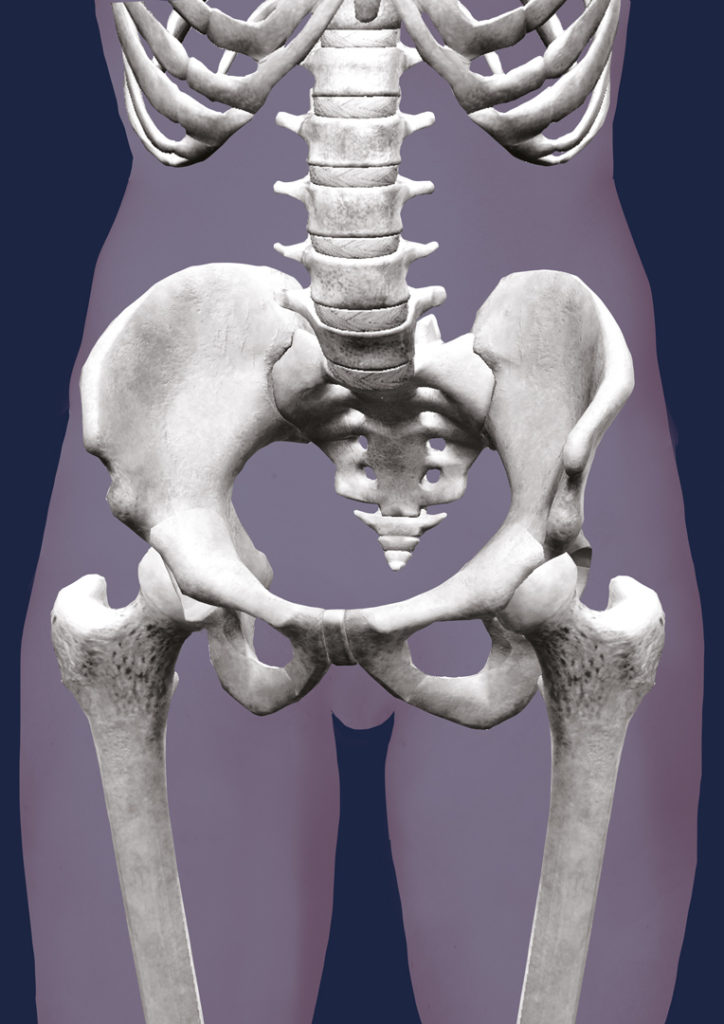
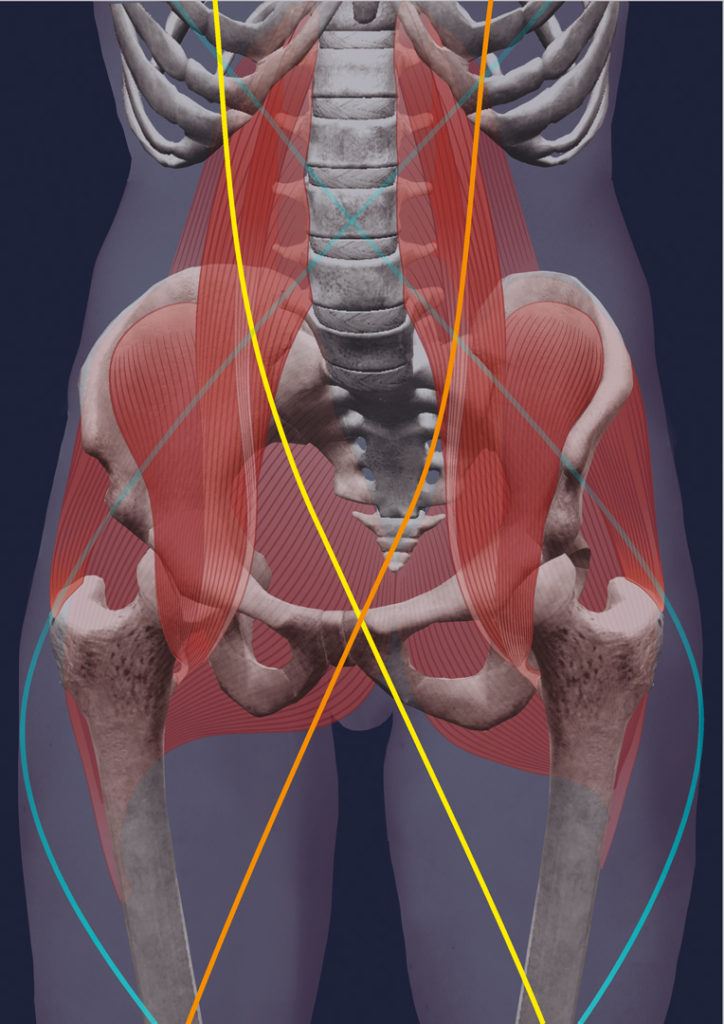
In terms of developmental kinesiology, this type of posture of the pelvis in flection is very probably caused by the persistence the so-called “new-born posture of the pelvis”. This is a posture of the pelvis in the first flection period. This quite short period is very important within the developmental kinesiology and for the subsequent development of the posture of the pelvis. Flection posture of the pelvis persists during the three months after birth as a relic of the intrauterine period (refer to the section about kinesiology of the intrauterine life). Abandonment of this type of posture and the onset of the first extension posture after the third month of life provide conditions for future normal posture of the pelvis and the corresponding configuration of the curve of the lumbar lordosis, posture of the hip joints including their angular parameters and the geometry of the femoral cervix. Persistence of the flection posture of the pelvis adversely influences the development of the lumbar spine hyperlordosis. Concurrently, insufficient development of thoracic kyphosis occurs, and insufficient development of the thoracic kyphosis is the main restriction for the upcoming normal development of the ribcage and the functionally related respiratory mechanics. On the other side, the ventral flection of the pelvis is manifested in the incorrect development of the hip joints in general as it restricts the correct centration of the head of the hip joint towards the acetabulum. Another severe developmental complication in terms of lateral deviation (hip joints stand in an uneven height) and axial rotation in the medial axis is the development of the symmetrical imbalance. Resulting deviation of the transversal pelvic axis towards the axis of the chest develops. This type of desaxation and lateral pelvic tilt are most probably the breaking point and original cause of the development of the scoliotic development of the spine. The following relative (functional) shortening of one lower limb is the remarkable facilitation of the development of the scoliosis.
-

The collapse of the arches of the feet, deviations of the axes of the calcanei, tarsal bones and digits
Illustration of the Solution
The patient and her mother regularly attended the therapeutic check-up visits, initially twice a month. After six months, we managed to fine-tune the therapeutic process and the visits were scheduled for once per month. After training, the mother ceased attempting to straighten her daughter by providing warnings since such an endeavour is utterly useless. Initially, there was a complication with the use of balance discs as the patient couldn’t tolerate them. She had considerable feelings of positional uncertainty, which wouldn’t subside as is usual in the majority of cases. The solution was found in the use of anti-slip mats that improved the adhesion of the support surfaces of the body of the patient and improved her feeling of certainty. To increase the intensity of the stimulation, the elastic bands appeared to be useful. The therapy led to gradual improvement in the autonomic regulation of the posture of the body. The hyperlordotic bending of the lumbar spine resolved. Afterwards, the thoracic spine arched, too. The tilting of the pelvis practically normalised and the abdominal wall returned to its physiological position. The posture of both girdles also got into physiological posture in the axis of the body.
-

Before the exercise using the Vojta method
-
Defective posture of the pelvis
-

After two years of intensive exercise
-

Physiological posture of the hips
Explanation of the Solution
The normalisation of the status of the impaired autonomic regulation of the posture of the body required an approach to this patient that would respect her positional uncertainty. Finding the way to perform the reflex with soft and balanced manner allowed the sufficient intensity of the stimulation. We have enabled the coordinated involvement of both straight and oblique muscular chains. Due to asthenic appearance of the patient and low tolerance of the lability of the support surfaces and the centres of gravity of the limbs, the use of highly adhesive mats proved to be optimal. Elastic bands were properly used as well. It is possible to increase their pressure against the performed movement, and they increase the comfort of stability. Therefore, we rather used these elastic bands instead of weights, which would be used with most patients. The weights on limbs significantly shift the centre of gravity of the limbs. This leads to a gradual increase in stimulation and, simultaneously, the reflex effort in balance normalisation increases too. The general development of the locomotive apparatus of the patient practically normalised. Thus, it is highly improbable that scoliosis could appear during future development.
Specific View of the Problem with the Persistence of the Ventral Posture of the Pelvis in the Childhood and Adolescence
The development of the skeleton of the locomotive apparatus is directly dependent on the preconditions, to which it has been prepared during the first year of life. The smooth course of the basic part of the psychomotor development is probably the most important event for the proper development of the musculoskeletal apparatus. Persistence of the ventral flection of the pelvis supposedly represents the greatest risk factor for the future impaired posture of the body. Lumbar vertebrae perform their essential function, i.e. they transfer the forces between the chest and the pelvis (upper and lower motion potential – refer to section on 3D biomechanics), with great problems, if not positioned physiologically. This impaired posture is most probably responsible for several functional disorders of the lumbar spine, including intervertebral disc herniation of this part of the spine. Reverse normalisation of the autonomic regulation of the posture of the pelvis into the physiological posture involves a therapeutic approach, which is concentrated on the voluntary analytical strengthening and stretching of the partial muscle groups. This approach has little hope for long-term success. The origin of this impaired posture lies in the disturbance of the basic motion program formed during the important period of the first year of life.
-

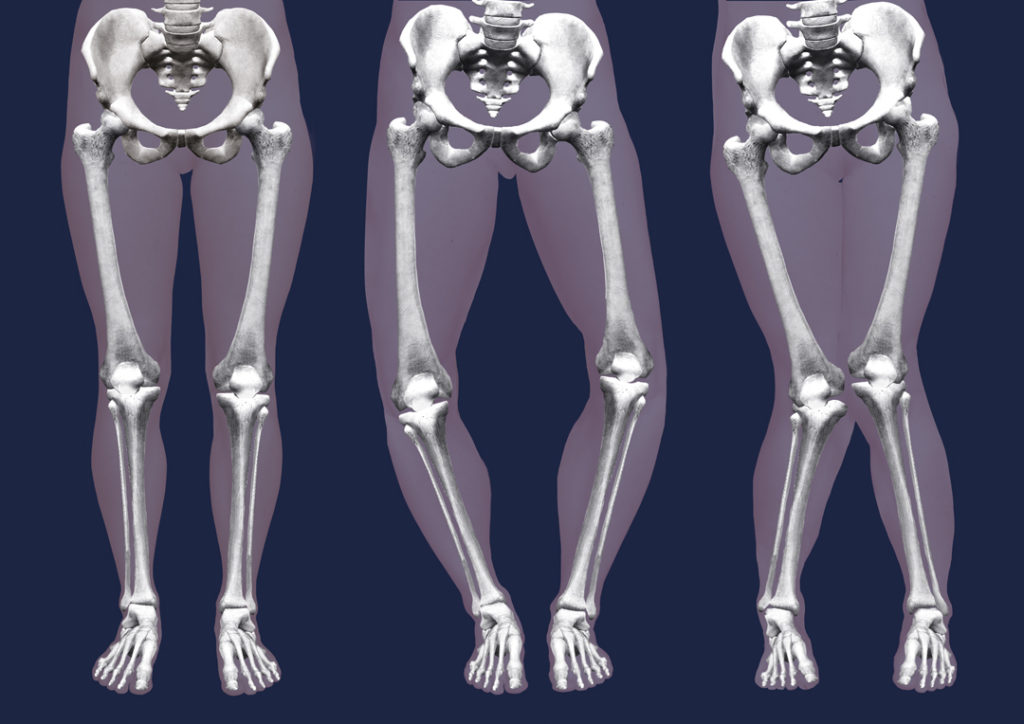
Deviation of the axes of the lower limbs -
Deviation of the axes of the lower limbs 
Deviation of the axes of the lower limbs
It’s this period which we should therapeutically “re-approach”, if we want to accomplish real improvements. This return could be practically implemented through reflex stimulation and the repair of the basic program of motor skills. Whatever went wrong during the first year of life, it must be repaired. The repair consists in two essential actions that work concurrently. The repair program is stimulated in a reflex way to restructure the basic program of motor skills (refer to the section on basic programs of motor skills). Along with the program repair, the musculoskeletal system itself is repaired as well. Only if the normalisation appears at the level of the program regulation of motor skills, could we expect the effect in terms of future good and smooth function of the locomotive apparatus. Then, the musculoskeletal apparatus would be able to endure the long-term exertion with physiological response and adequate time for regeneration.
-

Deviation of the axes of the lower limbs
-
Deviation of the axes of the lower limbs 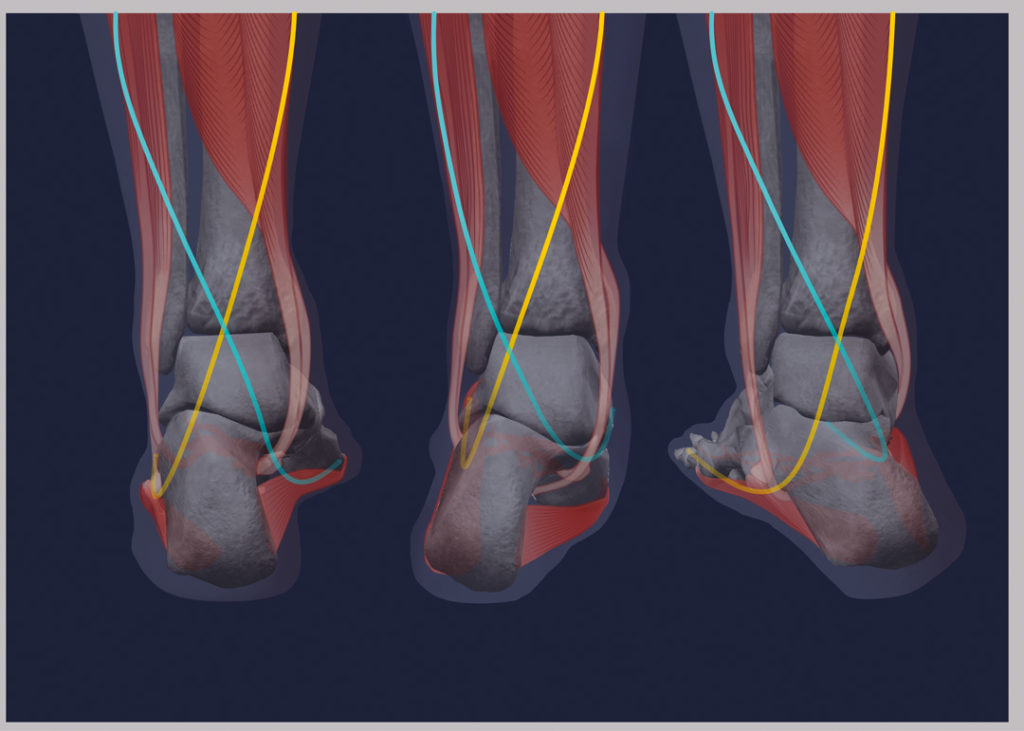
Deviation of the axes of the lower limbs
Disorders of the musculoskeletal apparatus are apparent in the defective posture of the body on all levels, and in the regulation of the basic stereotypical movements:
It is apparent in:
- The collapse of the arches of the feet, deviations of the axes of the calcanei, tarsal bones and digits
- Deviation of the axes of the lower limbs.
- Defective posture of the pelvis
- Impaired posture of the axes
of the spine - Disturbed configuration of the ribcage
- Pathological posture of the shoulder girdles
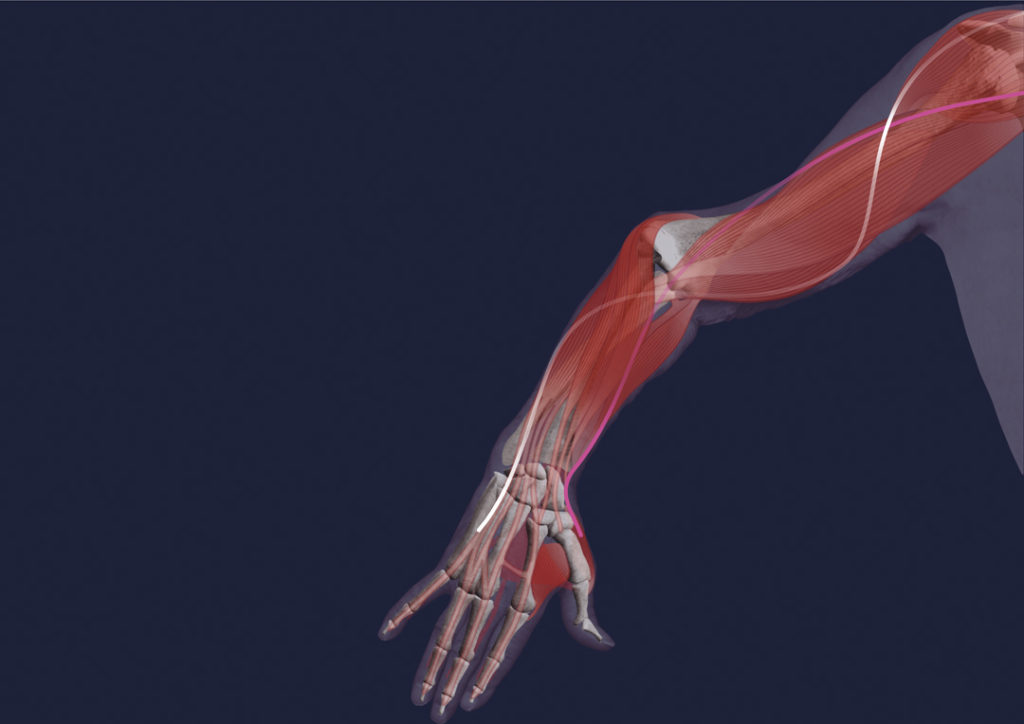
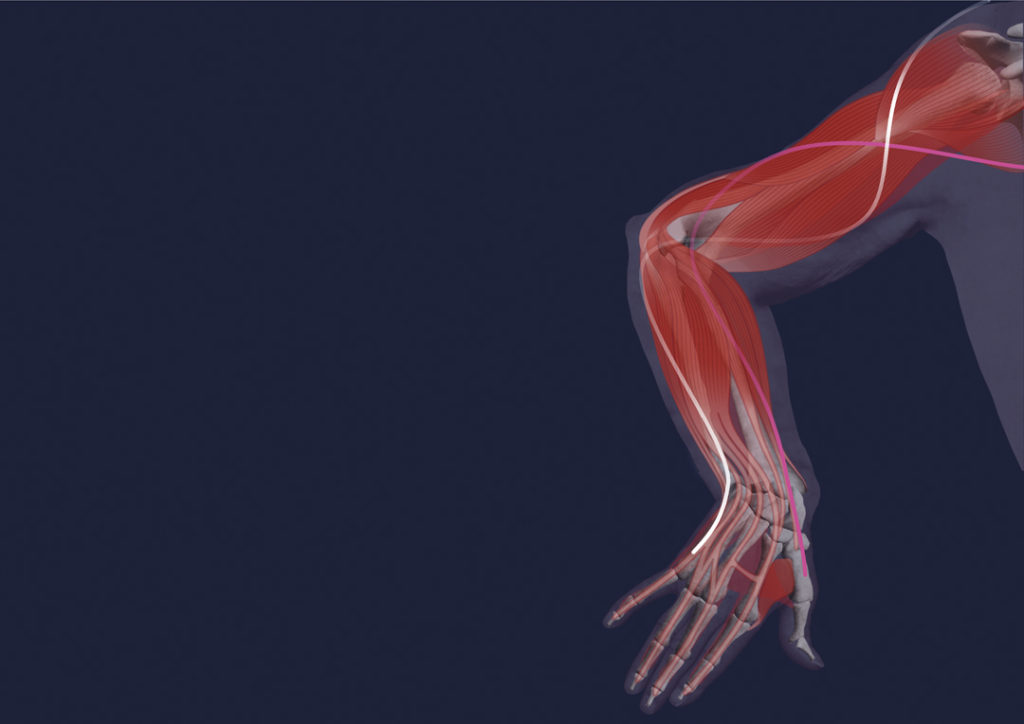
- Abnormal axes of the upper limbs and hand in particular
- Impaired posture of the head
- Impaired posture of the mandible
- Abnormal axes of the eye bulbs
- Collapse of the arches of the feet, deviations of axes of the calcanei, tarsal bones and digits
- Deviation from the axes of the lower limbs

General Kinesiology of Adults
Disorder of the kinesiology of the adults in terms of software impairment is most apparent in the pathology of the stereotypical movements:
- Gait
- Grasp
- Respiratory movements
- Stereotypical movements of the orofacial region, sucking, swallowing, speaking